Key words: osteolipoma, lipoma, variant
A 78-year-old female consulted for a ten-year gradually enlarging, right medial thigh mass, measuring 40 x 40 x 30 cm at the time of consultation. Physical examination showed right lower extremity external rotation, left lower extremity genu varum, and difficulty in walking due to mass effect. No imaging procedure was done. The patient was immediately scheduled for surgery after pre-operative clearance. Excision of the thigh mass was performed to relieve the patient of the mass effect. Intraoperative finding was a fibro-fatty mass located in the medial compartment of the thigh. There was neither attachment to the femur nor the major blood vessels. The mass was submitted for histopathologic examination.
Gross examination showed yellow to cream/yellow, ovoid, fibrofatty to firm tissue with cream/white to cream/yellow smooth, glistening cut sections, with patchy areas of calcifications and fibrosis. Histopathologic examination showed mature adipose tissue with admixed mature lamellar bone (Figure 1) and areas with hyaline cartilage undergoing ossification (Figure 2). The adipocytes were monotonous and monomorphic. There was no nuclear atypia, lipoblasts, mitotic activity, or necrosis seen. The case was signed out as osteolipoma.
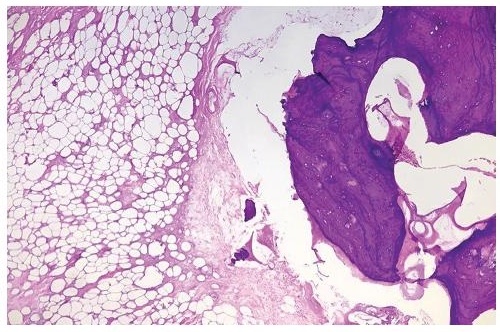
Figure 1. Mature adipose tissue with admixed mature lamellar bone (Hematoxylin & Eosin, 40x).
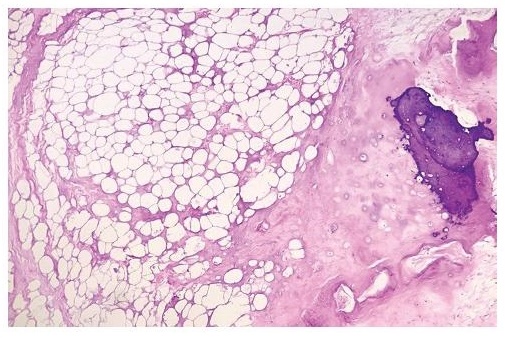
Figure 2. Mature adipose tissue with hyaline cartilage undergoing ossification (Hematoxylin & Eosin, 40x).
Lipomas are the most common benign soft tissue tumor occurring in subcutaneous tissues. Most patients are adults in their 30’s to 40’s. It is comprised of ma¬ture adipocytes without atypia.[1],[2] Variants of lipomas exist, having other mesenchymal components present, such as fibrous, smooth muscle, myeloid, chondral, vascular, or osseous tissue, admixed with the adipocytes. The nomenclature of the different variants depends on the type of tissue admixed with the adipocyte such as fibrolipoma, leiomyolipoma, myelolipoma, chondrolipoma, angiolipoma, and osteolipoma, respectively.[2] The rare variant osteolipoma is composed of mature lamellar bone interspersed within the adipose tissue.[3] Microscopically, they appear as predominantly mature adipose tissues with irregularly distributed mature lamellar bone with areas of ossification. This is the main morphologic criteria of the diagnosis.[4]
The principal pathologic differential diagnosis of a deep-seated lipoma is a well-differentiated liposarcoma. The latter is a deep-seated tumor common in adults above 50 years old. Morphologically, it is also composed of mature adipocytes. It is differentiated by the presence of scattered hyperchromatic nuclei, mostly situated within the fibrous septa.[5]
There are two main theories regarding the pathogenesis of osteolipoma: first, they may be directly derived from multipotent mesenchymal cells;[2] another, they may arise after repetitive trauma, ischemia, or metabolic changes initiating osseous metaplasia. The adipose tissue component strengthens this osteoblastic activity.[4],[6]
Osteolipomas have good prognosis similar with simple lipoma. Surgical excision is the recommended treatment.[1],[4]
[1] Cheng S, Lu SC, Zhang B, Xue Z, Wang HW. Rare massive osteolipoma in the upper part of the knee in a young adult. Orthopedics. 2012;35(9):e1434-7. PubMed DOI.
[2] Demiralp B, Alderete JF, Kose O, Ozcan A, Cicek I, Basbozkurt M. Osteolipoma independent of bone tissue: a case report. Cases J. 2009;2:8711. PubMed PubMed Central DOI.
[3] Fritchie KJ, Renner JB, Rao KW, Esther RJ. Osteolipoma: radiological, pathological, and cytogenetic analysis of three cases. Skeletal Radiol. 2012;41(2):237-44. PubMed DOI.
[4] Electricwala AJ, Panchwagh Y, Electricwala JT. Giant osteolipoma fixed to the greater trochanter of the femur in a seventy-year-old elderly woman. Cureus. 2017;9(2):e1036. PubMed PubMed Central DOI.
[5] Fisher C, Montgomery EA, Thway K. Biopsy interpretation of soft tissue tumors. Philadelphia: Lippincott Williams & Wilkins, 2011.
[6] Heffernan EJ, Lefaivre K, Munk PL, Nielsen TO, Masri BA. Ossifying lipoma of the thigh. Br J Radiol. 2008;81(1968):e207-10. PubMed DOI.