Background. The copper sulphate method, being economical, was used for hemoglobin screening in blood donation. Various references cite different number of tests that can be performed in a 100 mL copper sulphate solution.
Objective.The study was conducted to determine the effect of number of tests, hemoglobin level and working temperature on the specific gravity of 100 ml copper sulphate solution.
Methodology. Three groups of samples of known hemoglobin levels (<12 g/dl, 12-14 g/dl, and >14 g/dl) were tested using a 100 ml copper sulphate solution with specific gravity 1.053 at room temperature and at temperature of 29-30°C. Specific gravity of the solution was measured after every 5 tests for a total of 50 tests per experiment.
Result.There was no change in the specific gravity of copper sulphate solution used in 50 tests. There was no difference in the measured specific gravity across all experiments.
Conclusion. A 100 mL copper sulphate solution can be used for 50 tests using samples of various hemoglobin levels, at room temperature and at a higher temperature.
Key words: blood, hemoglobin, copper sulphate
The copper sulphate method for hemoglobin screening in blood donation has been in use for decades. The Far Eastern University-Nicanor Reyes Medical Foundation (FEU-NRMF) Medical Center, a tertiary hospital, previously utilized a colorimetric method using an automated analyzer for walk-in and mobile blood donation for potential blood donors until 2010, when it shifted to copper sulphate method to alleviate the cost of hemoglobin screening and the total cost of blood donor screening. The method is not only considered to be the most economical in FEU-NRMF and in the Philippines, but also in other developing countries.[1]
The copper sulphate method determines the hemoglobin content in a drop of blood by inference from the specific gravity of the copper sulphate solution. A drop of blood upon contact with the solution becomes encased in a sac of copper proteinate. The dispersion of the drop of blood and any immediate change in the specific gravity of the solution due to blood's dispersion is prevented for about 15 seconds.[2] The minimum hemoglobin requirement for blood donation is 12.5 g/dl and with a copper sulphate solution with specific gravity of 1.053, a drop of blood with hemoglobin of 12.5 g/dl or higher should sink in 10 to 15 seconds while a drop of blood with hemoglobin level of lower than 12.5 g/dl the drop of blood should float.[3]
An experimental study was conducted by doing experiments of adding another 25 drops of blood to a 100-ml copper sulphate solutions that have been used for 25 tests, one drop of blood per test, using samples of known hemoglobin levels at assigned working temperatures.
Subjects were chosen by judgment sampling. Individuals who were invited to participate in the study were blood donors who had undergone hemoglobin screening utilizing microcuvette technology (Hemocue) using capillary blood, and hospital employees with a recent complete blood count with low hemoglobin level. Possible subjects were given the option to participate or not to participate in the study. The details of the study were explained to them and they were given consent form. Those who accomplished the consent form were included in the study. Thirty subjects were chosen. Blood samples were extracted from the subjects and hemoglobin level of each sample was determined using a hemoglobin analyzer employing photometry as principle. Blood samples were grouped based on hemoglobin level, ten samples having hemoglobin level of less than 12 g/dl as one group, ten samples with 12 to 14 g/dl and remaining ten as one group with more than 14 g/dl.
The experiments in the study were conducted in the following order:
- Blood collection from subjects by a medical technologist
- Hemoglobin level determination of blood samples
- Grouping of blood samples as to three hemoglobin ranges
- Testing
- Recording of results
The copper sulphate solution used in the experiments was prepared by a medical technologist following the standard operating procedure of FEU-NRMF Medical Center which also conforms with the procedure stated in the USAID-published Anemia Detection Methods: A Manual for Health Workers. Please see appendix B and C for the preparation of the copper sulphate solution. The measurement of specific gravity of copper sulphate solution throughout the conduct of the study was performed by a medical technologist who did not perform any other part of the experiment.
Blood samples were collected by a medical technologist by venipuncture from each of the thirty subjects and transferred to tubes with spray-dried EDTA anticoagulant. Hemoglobin level of each blood sample was determined using a hemoglobin analyzer employing photometry as principle. Samples were grouped as to the three hemoglobin ranges, ten samples per group. Samples with hemoglobin level of less than 12 g/dl were assigned in group A, samples with hemoglobin level of 12 to 14 g/dl in group B and samples with hemoglobin level of more than 14 g/dl in group C. Each sample in the group was assigned with an accession number.
Six experiments were done. Experiments 1, 2 and 3 made use of samples from groups A, B and C, respectively and were conducted at room temperature. Experiments 4, 5 and 6 also made use of the same samples from groups A, B, and C, respectively, but were conducted at working temperature of 29ºC to 30ºC.
Each experiment was performed using 100 mL copper sulphate solution in a glassware with the buoy of the hydrometer that gave the solution a depth of 3 inches. One drop of blood was one test. Blood samples in the group were rotated to complete the 50 tests. As in the usual use of copper sulphate solution for hemoglobin screening, the drops of blood in the solution were observed for 15 seconds if they would sink or float. The specific gravity was 1.053 at the start of each experiment. Twenty-five tests were performed successively with no change in specific gravity of the solution measured after the twenty-fifth test. To complete the fifty tests, another 25 tests were performed and the specific gravity was determined after every 5 tests. The measurement of specific gravity was conducted by lifting the buoy of the hydrometer above the solution and lowering it into the solution with a light spinning motion. Once the buoy has stopped moving, the plane of the surface of the solution that intersected the scale on the stem of the buoy was taken as the specific gravity. Measurement of the specific gravity was done without any drop of blood touching the buoy of the hydrometer. The specific gravity in each measurement was recorded to determine if there would be change.
The investigator did not use any statistical test as the data could be analyzed without calculation. The measured specific gravity at the start of experiment, the specific gravity after the first twenty-five tests and every additional five tests to complete fifty tests were tabulated per experiment. Experiments 1, 2, and 3 are presented in table 1, and experiments 4, 5, and 6 in table 2.
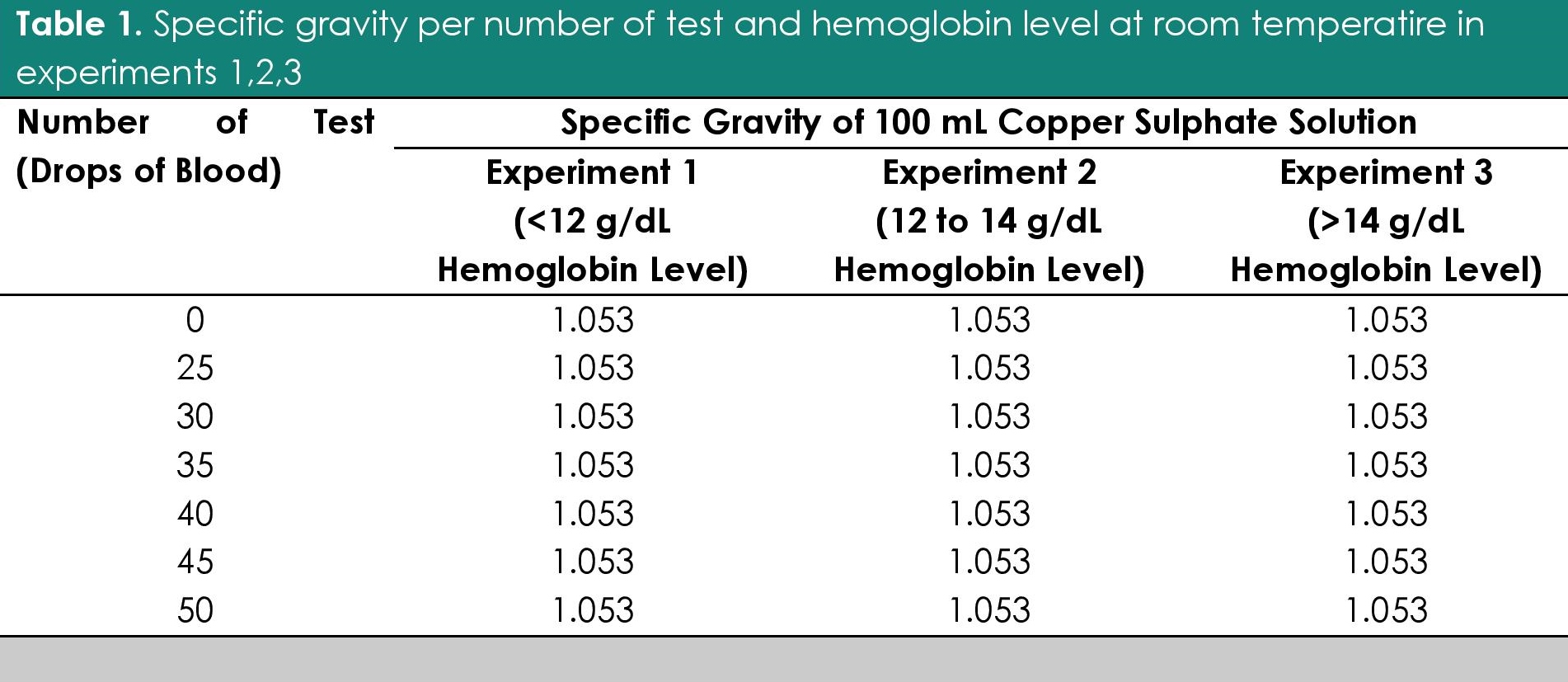
Table 1. Specific gravity per number of test and hemoglobin level at room temperature in experiments 1, 2 and 3
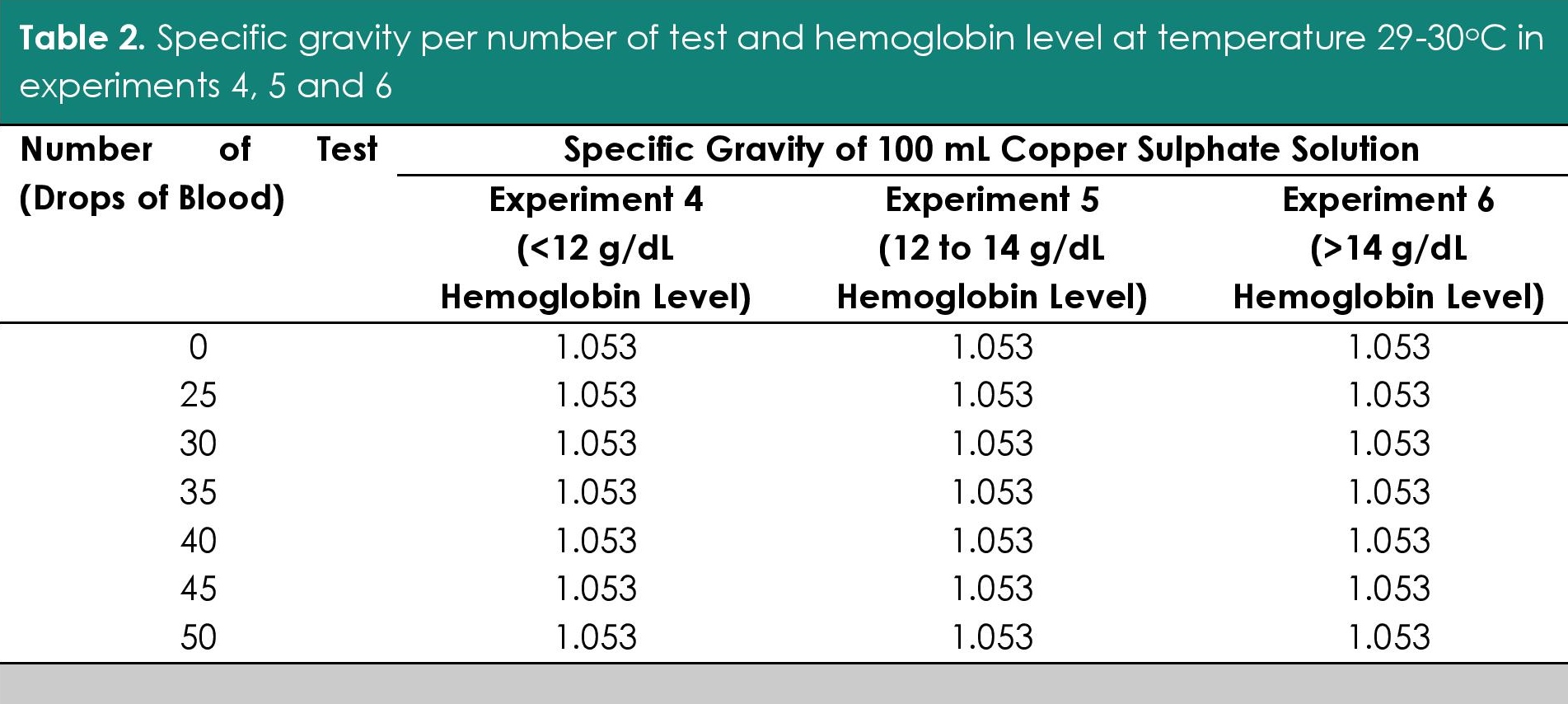
Table 2. Specific gravity per number of test and hemoglobin level at temperature 29-30ºC in experiments 4, 5 and 6
The change in specific gravity as to the number of tests was determined by observing for any increase in the specific gravity during performance of additional 25 tests in all six experiments.
The change in specific gravity as to hemoglobin level of the samples was determined by making a comparison of the measured specific gravity between experiments that used samples from groups with different hemoglobin ranges. Experiments 1 and 2, 2 and 3, 1 and 3, 4 and 5, 5 and 6, and 4 and 6 were compared.
The change in specific gravity as to temperature was determined by comparing the measured specific gravity between experiments 1 and 4, 2 and 5, and 3 and 6 which used samples belonging to same hemoglobin range but were conducted at different working temperatures.
There was no change in the specific gravity of 100 mL copper sulphate solution used for fifty tests in the six experiments (Tables 1 and 2). There was no difference in the measured specific gravity between experiments that were compared.
To maintain the sensitivity of the test, the United Kingdom Blood Transfusion and Tissue Transplantation Service, the World Health Organization in its publication entitled Model Standard Operating Procedure for Blood Transfusion Service and the American Association of Blood Banks recommend changing the solution after it has been used for 25 tests because the solution is expected to give unreliable results thereafter.[3],[4],[5] However, in the Anemia Detection Methods for Low Resource-Settings: A Manual for Health Workers published by USAID in 1997, the copper sulphate solution with the same specific gravity used for male patients in anemia screening recommends that it can be used for 50 tests.[6] The effect on the reliability of the test was not specified in the above stated publications if it is due to change in specific gravity secondary to the effect of temperature to the solution, the effect of hemoglobin content of the blood being tested or performance of more than 25 tests with one drop of blood per test. Although the solution changes in color after performance of several examinations, performance of 50 tests can be done in a 100-ml copper sulphate solution with no limitation in the visualization of blood dropped in the solution.
Phillips et al., in their article that introduced the copper sulphate method for hemoglobin screening, mentioned that correction for temperature is not needed during the testing as the coefficient of expansion of copper sulphate solution approximate closely those of blood and plasma but reports have been received by the California Blood Bank Society that the specific gravity of copper sulphate solution used in screening hemoglobin for potential blood donors change with temperature.[5]
The copper sulphate method of estimating hemoglobin has been thought by many to be an obsolete test due to the advent of new technologies. But due to the simplicity of the procedure and lower cost, the technique is still widely used even in the United Kingdom.[3] In the Philippines, the Philippine Blood Center still uses copper sulphate in donor screening for hemoglobin. Sawant et al., showed that 29% of potential donors who were deferred had hemoglobin level of more than 12.5 g/dl in a study involving 400 blood donors.[7] However, in the prospective study evaluating the quality and the cost of four hemoglobin screening methods, automated analyzer being the standard, done by Tondon et al., in 2009, they found out that the copper sulphate method still stands the test of time and remains the primary screening method.[1] They, however, recommended that to avoid the inappropriate deferrals, subsequent testing with Hemocue, a hemoglobinometer employing the photometer principle, should be done.[1]
The American Association of Blood Banks or AABB recommends 12.5 g/dl as the minimal hemoglobin requirement for an allogenic donor.[8] The FEU-NRMF Medical Center follows the recommendation of AABB for the minimal hemoglobin requirement for blood donation. In other countries, such as the United Kingdom, there are separate criteria for male and female donors, 12.5 g/dl for the former and 13.5 g/dl for the latter,[3] a recommendation also made by the United States Agency for International Development (USAID). AABB recommends the use of at least 30 mL working solution that will allow a drop of blood to fall approximately 3 inches after dropping (about 1 cm above the surface of the solution).[8] The USAID publication states that 100 mL of working solution should be used with no mention of the length that a drop should fall from the upper surface of the solution to the inner surface of the bottom of the container, with no recommended height of the fall of the drop of blood from the capillet to the surface of the solution.1 At the FEU-NRMF Medical Center, a 100 mL working solution in a 100 mL beaker is used for testing, giving the solution an approximate depth of 3 inches from the upper surface of the solution to the bottom of the container. The blood is dropped 1 cm above the surface of the copper sulphate solution.
The difference between the practice in FEU-NRMF Medical Center and the recommended standard operating procedures of the USAID (with the exception of the separate hemoglobin cut-off for non-pregnant females, the height of the fall of the drop of blood from the capillet to surface area of solution, and the depth that a drop of blood must sink from the surface of the solution to the bottom), is the number of drops of blood that can be tested in a 100 ml copper sulphate solution with specific gravity of 1.053. The standard operating procedure of FEU-NRMF Medical Center is to change the solution after 25 drops have been introduced which conforms with the Model Standard Operating Procedures for Blood Transfusion Service published by the World Health Organization and the Technical Manual of American Association of Blood Banks.[3],[4],[8] The USAID, however, has a different recommendation of using a 100 ml copper sulphate solution for 50 tests, which if proven to still maintain its specific gravity and therefore its sensitivity with the addition of another 25 tests in the same solution, will be of great benefit to blood banks that still use the method.[6]
Apart from the hemoglobin level of the blood, the working temperature and other proteins may interfere with the testing. Although it is said that correction for temperature is not needed because the coefficient of expansion of copper sulphate solution approximate closely those of blood and plasma.[5] Reports have been received by California Blood Bank Society in its e-Network Forum about the change in specific gravity with temperature.[2] Other proteins may also interfere and the outcome may be deleterious if an anemic donor will be bled. Such is the case of a patient who was bled with only 8 g/dl of hemoglobin, the patient passed the copper sulphate method due to hyperproteinemia secondary to multiple myeloma.[9] These other proteins in serum or whole blood may be tested using the same principle with copper sulphate method which means that they can influence the result of hemoglobin screening.[10] This is one of the limitations of Copper Sulphate method in hemoglobin screening. However, such a case has not yet been reported in FEU-NRMF Medical Center.
Two confounding variables were identified. One was the effect of the use of venous blood with liquid anticoagulant and not capillary blood. Since no study was found stating the difference between the weight of anticoagulated blood and blood without anticoagulant, it was assumed that the anticoagulant present in the blood collection tubes could affect the result of the experiment by diluting the blood. To minimize the possible error associated with the use of liquid anticoagulant, spray dried ethylene di-amine tetraacetic acid-anticoagulated (EDTA) lavender top tubes were used. During the conduct of the study, another confounding variable that was identified was the adherence of blood to the stem of the buoy of hydrometer, adding to the weight of the buoy, which caused a false decrease of the specific gravity. The plane of the surface of copper sulphate solution will intersect with a lower specific gravity number as the buoy becomes heavier. To resolve the problem, the other method of measuring specific gravity using refractometer was entertained, but was not employed as the method requires removal of drops of copper sulphate solution for the tests, decreasing the volume of the solution.
One limitation of the study is the conduct of experiments in only two working temperatures, room temperature, which is the recommended working temperature in blood banks and laboratories, and at a higher temperature of at least 29°C. Therefore, the study cannot make a recommendation for working temperature lower than that of room temperature.
This paper has shown that there is no change in the specific gravity of a 100 ml copper sulphate solution used for fifty tests with sample of various hemoglobin levels conducted at different working temperatures. Thus, a 100-mL copper sulphate solution can be used for fifty tests using samples of various hemoglobin levels at room temperature and at a higher temperature.
All authors certified fulfillment of ICMJE authorship criteria.
The authors declared no conflict of interest.
None.
[1] Tondon R, Verma A, Pandey P, and Chaudhary R. Quality evaluation of four hemoglobin screening methods in a blood donor setting along with their comparative cost analysis in an Indian scenario. Asian J Transfus Sci. 2009;3(2):66-9. DOI.
[2] Problems with QC of Copper Sulfate? E-Network Forum-California Blood Bank Society.
[3] Guidelines for blood transfusion services in the United Kingdom, 7th ed., UK blood transfusion and tissue transplantation services, 2005. Available online: https://www.gov.uk/government/uploads/system/uploads/attachment_data/file/228828/0117033715.pdf.
[4] Model standard operating procedures for blood transfusion service. World Health Organization, New Delhi, 2002. Available online: http://apps.searo.who.int/PDS_DOCS/B0235.pdf?ua=1.
[5] Philips RA, Van Slyke DD, Hamilton PB, Dole VP, Emerson K, Archibald RM. Measurement of specific gravities of whole blood and plasma by standard copper sulfate solution. J Biol Chem. 1950;183:305-30. Available online: http://www.jbc.org/content/183/1/305.full.pdf+html.
[6] Anemia detection methods in low-resource settings: a manual for health workers. Seattle, Washington, USA: PATH Publications, 1997. Available online: http://www.path.org/publications/files/TS_anemia_guide_health_workers.pdf.
[7] Sawant RB, Bharucha ZS, Rajadhyaksha SB.Evaluation of hemoglobin of blood donors deferred by copper sulfate method for hemoglobin screening. Transfus Apher Sci. 2007;36(2):143-8. PubMed DOI.
[8] Brecher ME, American Association of Blood Banks. Technical Manual, 15th ed. Bethesda, Md.: American Association of Blood banks, 2005. Available online: http://www.eqas.ir/pdf/lib/AABB%20Technical%20Manual%2015TH.pdf.
[9] Mannarino AD, Macpherson CR. Copper sulfate screening of blood donors: report of a donor passing the test with less than eight grams of hemoglobin. Transfusion:1963;3:398-400. PubMed.
[10] McPherson RA, Pincus MR, Henry JB. Henry's clinical diagnosis and management by laboratory methods, 21st ed., Philadelphia: Saunders Elsevier, 2007. NLIM ID: 101289889 [Book].