Key words: ameloblastic, fibroma, odontoma
A seven-year-old male was referred for consult at the oral & maxillofacial surgery & implantology section of the hospital due to a large asymptomatic left maxillary mass resulting to a noticeable facial asymmetry. Clinical examination showed a solitary bony hard swelling on the left posterior maxilla exhibiting buccal and palatal expansion. Tooth mobility of the left premolars and absent permanent molar are likewise noted (Figure 1). CT scan showed an enlarging mass on the left posterior maxilla exhibiting an amorphous ovoid opacity surrounded by a defined radiolucent border overlying the crown of a permanent molar displacing the maxillary sinus floor without perforating it. (Figure 2) Based on the initial diagnostics considered impressions where ameloblastic fibro-odontoma and calcifying epithelial odontogenic tumor. Patient was admitted, prepared, once cleared underwent surgical enucleation of the mass under GETA via an intra-oral Lefort 1 incision, the mass was then submitted for histopathologic examination. 11 months after the operation (Figure 3), both clinical and radiographic findings show no sign of recurrence.

Figure 1. Clinical appearance. Mass producing facial asymmetry on left side of the patient, intra oral finding showing an evident bony hard mass on the posterior region of the left maxilla with noticeable altered eruption pattern of the left permanent molars.
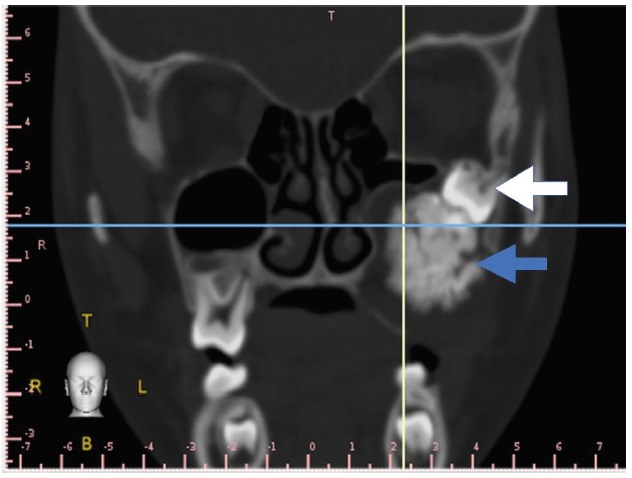
Figure 2. Coronal cut CT scan showing impacted permanent molar and large amorphous opacity surrounded by a defined radiolucency.

Figure 3. Clinical appearance 11 months post-operatively showing improvement in facial symmetry and defect on the operative site with no clinical sign of recurrence.
Histologic examination revealed a benign tumor composed of ameloblastic islands amidst a cellular fibrous background (Figure 4), and areas showing dentin formation. (Figure 5). Histomorphologic features were consistent with an ameloblastic fibro-odontoma.
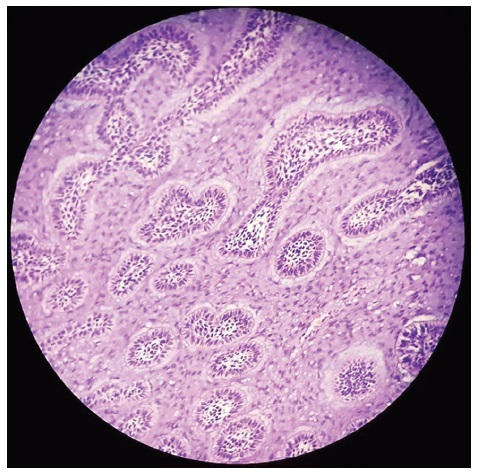
Figure 4. Ameloblastic islands in a fibromyxoid background (H & E, 40x).
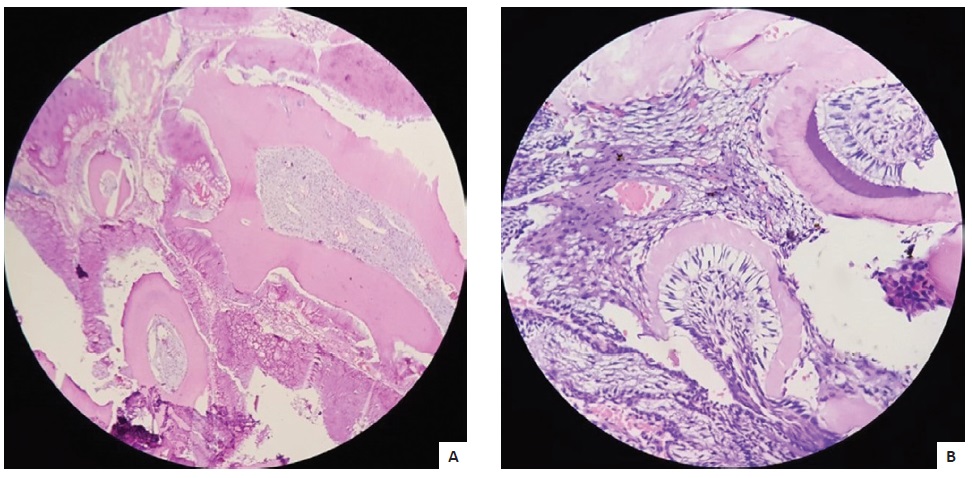
Figure 5. Areas with dentin formation (H & E, [A], 40x and [B], 100x).
As listed in the updated 2017 WHO classification of benign odontogenic tumors and cyst, a handful are considered calcifying types of epithelial or mixed lesions.[1] In a review by Augello et.al. regarding AFO the prevalence is set at 1-3.4% among odontogenic tumors with no gender predilection equally found on either jaw but is seen more occurring in the molar regions also associated with an impacted tooth.[2] Generally seen with a mean age of 11.5 years which together with the complaint of an asymptomatic growing mass together with the distinct calcification on diagnostic imaging can be considered an important criterion for considering AFO.[2] AFO is currently recognized as part of the histologic spectrum of developing odontomas, although it is argued that in some cases of AFO neoplastic changes may be possible specially with large AFO.[3]
AFO has histologic features identical to ameloblastic fibroma (AF) with a hard tissue component consisting of dental hard structures.1 The AF component is the “soft tissue” component”, while the “hard tissue” component contains a calcifying component composed of enamel and dentin structures.[1],[4] AFO is described in its WHO (World Health Organization) classification as a lesion similar to AF, and both have been defined as hamartomatous lesions, believed to be stages of odontoma formation.[2],[5] Similar to what most authors suggest this case of a large AFO was primarily managed conservatively with enucleation, reserving more ablative surgery for rare cases of recurring AFO as well as confirmed malignant transformations.
Patient consent was obtained before submission of the manuscript.
All authors certified fulfillment of ICMJE authorship criteria.
The authors declared no conflict of interest.
None.
[1] Barnes L, Eveson, JW, Reichart P, Sidransky D, eds. WHO Classification of Tumours, Pathology and Genetics of Head and Neck Tumours. Lyon, France, 2005.
[2] Augello M, Rabufetti A, Ghazal G, Yurtsever H, Leiggener C. Ameloblastic fibro-odontoma in children. Clinical aspects and review of literature. Oral and Maxillofacial Surgery Cases. 2017;3(2):34-41. CrossRef
[3] Wright JM, Vered M. Update from the 4th edition of the World Health Organization classification of head and neck tumours: Odontogenic and maxillofacial bone tumors. Head Neck Pathol. 2017;11(1):68-77. PubMed PubMed Central CrossRef
[4] Martinez A. Mandible/maxilla benign tumors/tumor-like conditions odontoma. Retrieved from http://www.pathologyoutlines.com/topic/mandiblemaxillaodontoma.html
[5] Kumar LKS, Manuel S, Khalam SA, Venugopal K, Sivakumar TT, Isaac J. Ameloblastic fibro-odontoma. Int J Surg Case Rep. 2014;5(12):1142-4. PubMed PubMed Central CrossRef